
As a pelvic health physical therapist and sexuality counselor, my work lives at the intersection of patient care and provider education. In my experience as an assistant professor of women’s health within medical education, I’ve led clinical education and contributed to multidisciplinary training and program development across medical, residency, and fellowship programs. Through that work, I’ve seen how pelvic health concerns are identified in practice—and where opportunities for earlier intervention are often missed—even in really good care.
Primary care providers are the front door to pelvic health.
You are often the first person patients trust with symptoms that feel confusing, frustrating, or honestly… a little awkward to bring up.
Because the reality is—many people, especially women and non-binary folks, wait years to talk about:
- Sexual dysfunction (pain, libido, orgasm, etc.)
- Urinary dysfunction
- Bowel dysfunction
- Prolapse
- Pelvic pain
- Changes that started after childbirth, surgery, or menopause
Not because they don’t care. But because they don’t always know it’s something they can—or should—bring up. And when those concerns aren’t addressed early, they don’t just go away. They adapt and more often than not, become more complex.
The Pelvic Health Care Gap
Pelvic floor dysfunction is common, multifactorial, and often progressive—affecting nearly one-third of women in primary care settings—yet screening and treatment don’t consistently reflect that reality (Kenne KA, Wendt L, et al., 2022).
Many providers report only sometimes screening for urinary symptoms, and rarely for prolapse or sexual concerns. There is also limited awareness of referral pathways and first-line management (Weimer A, et al., 2024). And when patients are referred, about half receive no treatment prior to specialty care (Prentice A, et al., 2019).
This is not because providers aren’t paying attention. It reflects a combination of factors: limited time, gaps in training, uncertainty about scope, and broader structural barriers within the healthcare system (Mazloomdoost D, et al., 2018; Wong JW, et al., 2019).
When access to care is limited—whether due to insurance coverage or referral availability—it doesn’t just affect treatment. It can shape whether providers feel equipped to open the door to these conversations in the first place.
As a result, patients often wait years before these issues are addressed.
What may begin as mild or intermittent symptoms can evolve into more complex, overlapping pelvic floor disorders—bladder, bowel, and sexual dysfunction that become increasingly difficult to treat over time. Untreated symptoms in one system can contribute to dysfunction across others, creating compounding patterns that require more intensive and prolonged care.
As patients adapt, the body adapts:
- Musculoskeletal and neuromuscular changes (including altered tone and peripheral sensitivity)
- Changes in pain processing, including central sensitization and shifts in neurochemical and hormonal signaling
- Motor control changes and reduced tolerance to movement and load
Now we’re treating complexity—not just a symptom.
This progression is associated with longer recovery, increased healthcare utilization, and a higher risk of functional limitation and disability—when earlier recognition and intervention could have significantly changed the trajectory.
Decision-Making Framework & The Role of Pelvic PT
The big picture: multidisciplinary care is the gold standard
Pelvic floor dysfunction is rarely isolated—it’s multifactorial and multicompartmental.
That’s why multidisciplinary care is the gold standard for pelvic floor dysfunction.
And within that model, pelvic health physical therapists (PTs) are central; not adjunct (Tsai TY, et al. 2025) (Wallace SL, et al. 2019)
Pelvic PTs are uniquely trained to assess and treat this full system—integrating:
- Musculoskeletal and neuromuscular function
- Movement and biomechanics
- Pain science
- Behavioral strategies
- An understanding of the multifactorial nature of pelvic floor dysfunction, including colorectal, urologic, gynecological, and other system contributions that shape clinical presentation
And importantly, care is delivered through a biopsychosocial lens, recognizing that pelvic and sexual health are shaped by more than just anatomy.
There is very strong evidence positioning pelvic PT as a first-line, minimally invasive, and effective treatment for many pelvic floor disorders—especially when integrated early as part of a multidisciplinary care team. Pelvic PT isn’t extra care. It is the care.
A very recent 2026 study found that many patients with persistent “UTI” symptoms—despite negative cultures—had:
- vestibulodynia (85%)
- pelvic floor hypertonicity (75%)
Meaning this may not be just a bladder issue—it may be a pelvic system issue.
What Can You Do Right Now? (Screening for Pelvic Floor Dysfunction in Primary Care)
1. Screen every patient for pelvic floor symptoms—not just the ones who bring it up.
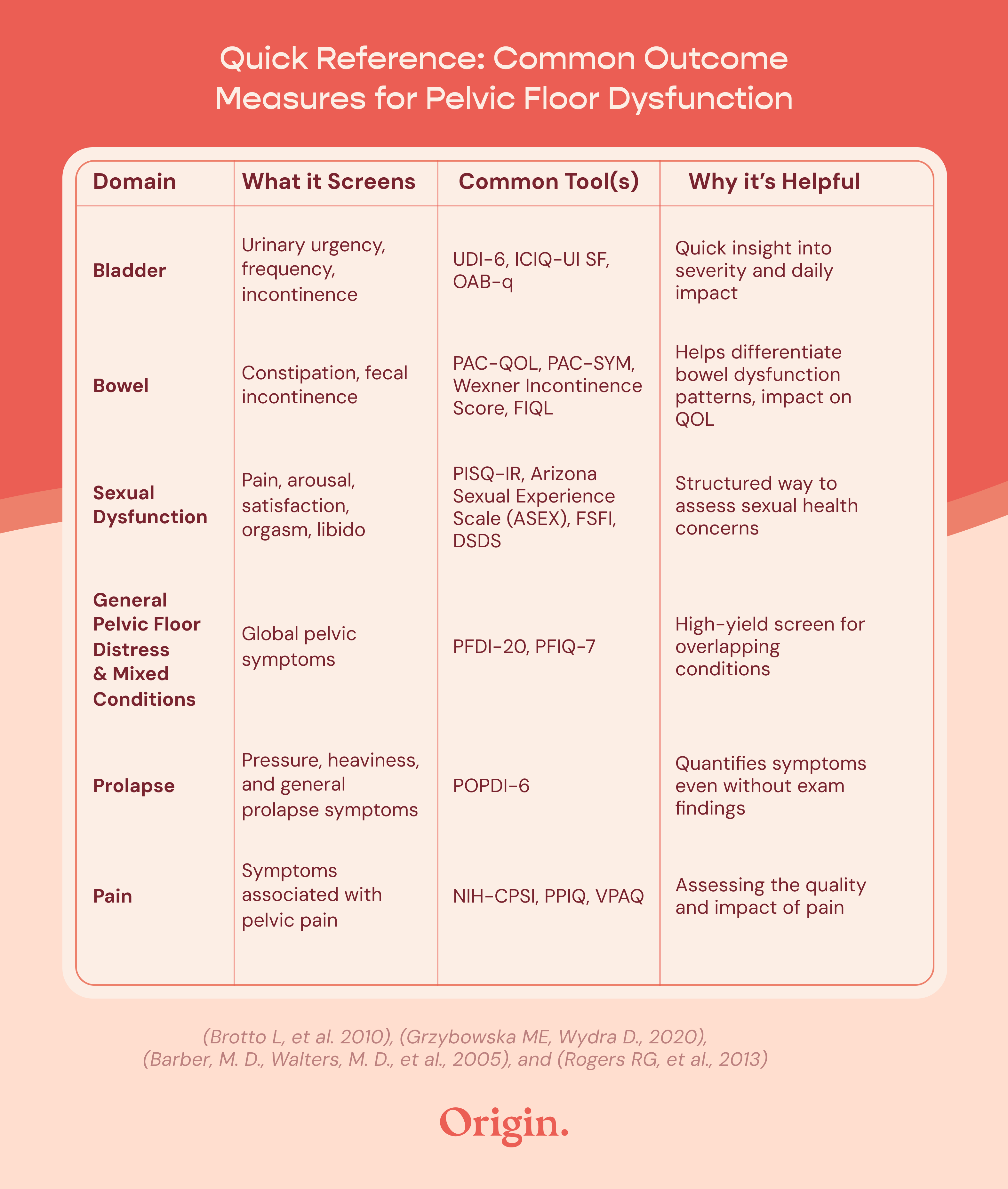
A few simple questions about bladder, bowel, and sexual health—paired with a validated outcome measure when appropriate—can quickly give you direction as a provider and validation for your patient.
Sample screening questions:
- “Do you ever leak urine when you cough, sneeze, laugh, exercise, or during sex?”
- “Do you feel a strong urge to urinate that’s hard to control?”
- “Do you feel heaviness, pressure, or a sensation of something falling in the vaginal area?”
- “Any constipation or difficulty controlling your bowels?”
- “Do you have a history of low back, hip, or groin pain that impacts your daily activity?”
- “Are you noticing any changes in your sexual function?”
Used together, screening questions and validated outcome measures help you identify concerns earlier, guide intervention planning, track progress over time, and bring structure to conversations that can otherwise feel difficult to navigate—enhancing the clinical conversation rather than replacing it (Brotto L, et al. 2010).
2. Use structure to guide the conversation and next steps
You don’t need to go deeper—you need to go structured.
Two frameworks can help (Anon, 1976) (Cicek OS, et al 2024):
PLISSIT / EX-PLISSIT (how to respond in the moment)
- Give permission
- Provide brief, relevant information
- Offer one clear next step
- Permission is ongoing—not a one-time step. With EX-PLISSIT, you return to permission at each stage of the conversation, reinforcing safety and openness as the discussion evolves.
ICSM (how to organize clinical decision-making)
The International Consultation on Sexual Medicine (ICSM) outlines a 5-step approach (Hatzichristou D, et al 2016):
- Basic evaluation (medical, sexual, psychosocial)
- Determine need for further assessment or referral
- Provide patient education
- Initiate treatment or referral
- Follow up
This provides a clear pathway, even in time-limited visits.
3. Refer to pelvic physical therapy early
Early referral helps:
- Prevent progression from acute → chronic
- Reduce symptom complexity
- Improve patient outcomes
- Decreases the financial burden for managing a chronic illness
4. When time is limited: making space without derailing the visit
Pelvic floor and sexual health concerns are often raised at the end of the visit, and they deserve more than a rushed response. You don’t have to address everything in that moment.
A practical approach (Perelman M., 2018):
- Briefly listen to understand the concern
- Normalize and validate
- Acknowledge time constraints while reinforcing importance
- Plan next steps: schedule follow-up and/or initiate referral with brief education
This approach allows you to respect both the time you have and the complexity of the concern—while ensuring the patient feels heard and has a clear next step.
The Takeaway
These steps are not about “doing more”.
It’s about doing the right amount—at the right time—within your role.
And when you combine PFD screening questions with frameworks like PLISSIT, ICSM, and validated outcome measures, it becomes part of a system that helps you move from: “I’m not sure how to approach this” to “I know exactly what my next step is.”
When to Consider Pelvic Floor Physical Therapy
Pelvic PT is first-line, conservative management for pelvic floor dysfunction across all genders.
Refer for:
- Pelvic girdle pain (including pregnancy/postpartum and menopause)
- Urinary or fecal incontinence, urgency/frequency
- Constipation or difficulty with bowel movements
- Sexual dysfunction (dyspareunia, genital pain, orgasm dysfunction, erectile dysfunction)
- Chronic pelvic pain (vulvodynia, interstitial cystitis/painful bladder syndrome, endometriosis-related pain)
- Diastasis recti
- Athletes with pelvic floor symptoms (e.g., leakage, pain, pressure)
- Oncology patients with pelvic floor dysfunction (e.g., post-treatment pain, incontinence, fatigue)
Access & What Partnering with Origin Looks Like
Access is one of the biggest barriers in pelvic health.
Origin helps bridge that gap through:
- In-person care
- Virtual care
- Hybrid care models
- Insurance coverage
Virtual care lowers the barrier to entry—which is often the hardest step.
Conclusion
Closing the pelvic health gap doesn’t require overhauling your practice.
Many gaps in care stem from under-recognition, limited training, and delayed referral. Recognizing common presentations, naming pelvic floor dysfunction, and referring early for first-line conservative care can significantly improve outcomes.
Next Steps
If you’re looking to simplify pelvic health referrals, Origin offers tools and resources to support your workflow—including referral pathways and care coordination support.
Because when providers feel supported, patients feel it too.
Sources:
Barber, M. D., Walters, M. D., et al. (2005). "Short forms of two condition-specific quality-of-life questionnaires for women with pelvic floor disorders (PFDI-20 and PFIQ-7)." American Journal of Obstetrics and Gynecology 193(1): 103-113
Brotto LA, Bitzer J, Laan E, Leiblum S, Luria M. Women's sexual desire and arousal disorders. J Sex Med. 2010 Jan;7(1 Pt 2):586-614. doi: 10.1111/j.1743-6109.2009.01630.x. Erratum in: J Sex Med. 2010 Feb;7(2 Pt 1):856. PMID: 20092454
Cicek Ozdemir S, Dogan Gangal A, Senturk Erenel A. The Effect of Sexual Counseling Based on PLISSIT and EX-PLISSIT Models on Sexual Function, Satisfaction, and Quality of Life: A Systematic Review and Meta-Analysis. Arch Sex Behav. 2024 Oct;53(9):3485-3513. doi: 10.1007/s10508-024-02898-2. Epub 2024 Jun 18. PMID: 38890226; PMCID: PMC11390780
Kenne KA, Wendt L, Brooks Jackson J. Prevalence of pelvic floor disorders in adult women being seen in a primary care setting and associated risk factors. Sci Rep. 2022 Jun 14;12(1):9878. doi: 10.1038/s41598-022-13501-w. PMID: 35701486; PMCID: PMC9198100
Grzybowska ME, Wydra D. Responsiveness of two sexual function questionnaires: PISQ-IR and FSFI in women with pelvic floor disorders. Neurourol Urodyn. 2021 Jan;40(1):358-366. doi: 10.1002/nau.24568. Epub 2020 Nov 4. PMID: 33150611
Hatzichristou D, Kirana PS, Banner L, Althof SE, Lonnee-Hoffmann RA, Dennerstein L, Rosen RC. Diagnosing Sexual Dysfunction in Men and Women: Sexual History Taking and the Role of Symptom Scales and Questionnaires. J Sex Med. 2016 Aug;13(8):1166-82. doi: 10.1016/j.jsxm.2016.05.017. PMID: 27436074
Mazloomdoost D, Crisp CC, Kleeman SD, Pauls RN. Primary care providers' experience, management, and referral patterns regarding pelvic floor disorders: A national survey. Int Urogynecol J. 2018 Jan;29(1):109-118. doi: 10.1007/s00192-017-3374-8. Epub 2017 May 25. PMID: 28547268
Prentice A, Bazzi AA, Aslam MF. Treatment patterns of primary care physicians vs specialists prior to subspecialty urogynaecology referral for women suffering from pelvic floor disorders. World J Methodol. 2019 Jun 28;9(2):26-31. doi: 10.5662/wjm.v9.i2.26. PMID: 31367545; PMCID: PMC6658364
Rogers RG, Rockwood TH, Constantine ML, Thakar R, Kammerer-Doak DN, Pauls RN, Parekh M, Ridgeway B, Jha S, Pitkin J, Reid F, Sutherland SE, Lukacz ES, Domoney C, Sand P, Davila GW, Espuna Pons ME. A new measure of sexual function in women with pelvic floor disorders (PFD): the Pelvic Organ Prolapse/Incontinence Sexual Questionnaire, IUGA-Revised (PISQ-IR). Int Urogynecol J. 2013 Jul;24(7):1091-103. doi: 10.1007/s00192-012-2020-8. Epub 2013 Apr 30. PMID: 23632798
Perelman M. Sex Coaching for Non-Sexologist Physicians: How to Use the Sexual Tipping Point Model. J Sex Med 2018;15:1667e1672
Ross S, Fast H, Garies S, Slade D, Jackson D, Doraty M, Miyagishima R, Soos B, Taylor M, Williamson T, Drummond N. Pelvic floor disorders in women who consult primary care clinics: development and validation of case definitions using primary care electronic medical records. CMAJ Open. 2020 May 28;8(2):E414-E419. doi: 10.9778/cmajo.20190145. PMID: 32467289; PMCID: PMC7269601
Tsai TY, Huang SH, Liao CK, Tsai KY, Hsieh PS, Chiang SF, Hiraike O. Multidisciplinary Team Approach to Pelvic Floor Disorders: A Systematic Review. Biomed J. 2025 Sep 8:100912. doi: 10.1016/j.bj.2025.100912. Epub ahead of print. PMID: 40930419
Wallace SL, Miller LD, Mishra K. Pelvic floor physical therapy in the treatment of pelvic floor dysfunction in women. Curr Opin Obstet Gynecol. 2019 Dec;31(6):485-493. doi: 10.1097/GCO.0000000000000584. PMID: 31609735
Weimer A, Hallock JL, Chen CCG. Primary care providers practice patterns regarding female pelvic floor disorders. Fam Med Community Health. 2024 Mar 14;12(1):e002448. doi: 10.1136/fmch-2023-002448. PMID: 38485284; PMCID: PMC10941109
Wong JW, Kaneshiro BE, Oyama IA. Primary Care Physician Perceptions of Female Pelvic Floor Disorders. Hawaii J Med Public Health. 2019 Apr;78(4):132-136. PMID: 30972236; PMCID: PMC6452021




